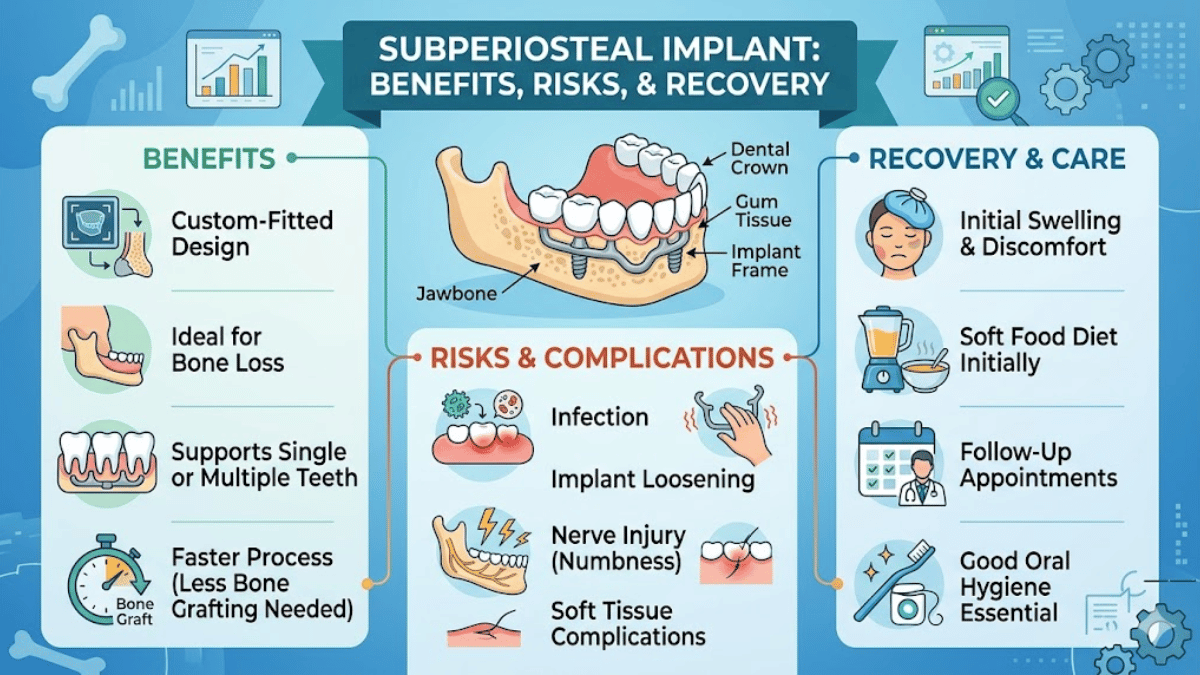
I would answer the core question this way: a subperiosteal implant is a custom-made dental implant framework that rests on top of the jawbone, beneath the periosteum, instead of being drilled into the bone like a conventional endosteal implant. It is mainly used for people with severe jaw atrophy who are poor candidates for standard implants or who want to avoid major bone-grafting surgery. Modern versions are digitally planned from CBCT scans, manufactured in titanium, and fixed in place with screws or other stabilizing features before supporting a bridge or denture.
That description sounds almost simple. In practice, the treatment sits at the intersection of oral surgery, prosthodontics, biomaterials, and patient selection. Subperiosteal implants are not the first choice for most people missing teeth. Endosteal implants, which heal inside bone, remain the standard approach when bone volume is sufficient. But for patients with severely resorbed jaws, especially older adults or medically complex patients who cannot tolerate grafting, subperiosteal systems have become newly relevant in the digital era.
Their history explains both their promise and their controversy. Subperiosteal implants were widely used from the 1940s through the 1980s, then fell out of favor as root-form endosseous implants delivered more predictable long-term outcomes. Now, advanced imaging, CAD/CAM planning, direct metal laser sintering, and customized fixation have revived interest. The modern question is no longer whether the concept exists. It is whether the newer, more precise version can offer stable, humane, lower-morbidity treatment for the small group of patients who truly need it.
What a subperiosteal implant actually is
I think the easiest way to picture a subperiosteal implant is to imagine a titanium framework shaped to the contours of an individual patient’s jaw. Rather than disappearing into the bone as a screw implant does, the frame lies on the bone surface under the periosteum, with posts or abutment connections emerging through the soft tissue to support the prosthetic teeth. In contemporary practice, the framework is usually designed from cone-beam CT data and refined in digital software so that its contact points, emergence profile, and fixation sites correspond to the patient’s anatomy.
That custom fit is the whole point. A patient with pronounced alveolar resorption may have too little vertical height or width for ordinary implants, even after considering short or tilted implants. In those cases, a subperiosteal design offers a graft-sparing alternative. A 2025 review described these devices as implants “placed on the bone surface rather than within it,” a distinction that captures why they are reserved for anatomically difficult cases rather than routine tooth replacement.
An oral-surgery review noted that “digital imaging, 3D printing, and customized implant design” have “significantly improved treatment options” for severe bone deficiency.
Why they disappeared, and why they are back
I find the history of subperiosteal implants especially revealing because it is a story of both ingenuity and overreach. Early versions were commonly used for atrophic jaws in the 1940s to 1980s, often fabricated from Vitallium and made through more cumbersome impression-based techniques. But once Brånemark-style endosseous implants established themselves in the 1980s, the older systems looked less predictable. Hardware exposure, mobility, recurrent inflammation, pain, and soft tissue breakdown repeatedly pushed the method to the margins of implant dentistry.
The revival has been driven not by nostalgia but by engineering. Modern systems are usually titanium, digitally designed, and additively manufactured. Their fixation can be improved with strategically placed screws into preserved buttresses or thick cortical regions, and the fit is far more precise than what earlier generations could routinely achieve. That does not erase the biological risks, but it changes the surgical proposition. A 2024 systematic review of additively manufactured subperiosteal implants found 97.8 percent of implants still functioning after a weighted mean follow-up of 21.4 months, though soft-tissue exposure and infection remained important complications.
The reappearance of these implants, then, is not a return to the past. It is an attempt to solve a persistent problem, the severely atrophic jaw, with better tools than previous generations had.
Who is actually a candidate
I would not describe subperiosteal implants as an alternative for everyone who wants faster treatment. They are best understood as a niche option for a specific clinical population: patients with advanced jawbone loss, often edentulous or nearly edentulous, who lack the bone volume needed for conventional implants and either cannot undergo, or do not want, extensive grafting. Reviews consistently place them in the setting of severe alveolar atrophy, especially when standard-size implants are not feasible.
That group may include older adults with long-term denture wear, patients whose previous implants failed with progressive bone resorption, and some post-traumatic or post-oncologic cases. In the six-year follow-up study published in 2024, inclusion criteria included severe atrophy, inability to place standard implants, and opting out of regeneration procedures. Exclusion criteria included uncontrolled diabetes, immunocompromised states, poor oral hygiene, tobacco use, bruxism, and the presence of anatomy suitable for conventional implants.
The strongest reason to consider the technique is not convenience alone. It is the combination of anatomy and risk. Some patients need fixed teeth but are poorly served by repeated grafting, long treatment windows, or high-morbidity reconstruction. For them, the question becomes whether a custom surface implant can restore function with acceptable complication risk.
How the modern procedure is planned and placed
I would describe the modern workflow as heavily digital before it is surgical. The patient first undergoes three-dimensional imaging, usually CBCT, to map the residual bone and identify where fixation is realistic. Engineers or dental technicians then convert DICOM data into an STL model, refine the bony contours in software, and design both the implant framework and, in many protocols, the surgical guide. The implant is then produced from titanium alloy, commonly by additive manufacturing.
In surgery, the clinician raises a flap to expose the bone surface, seats the custom frame, and secures it with self-drilling or preplanned osteosynthesis screws. In the 2024 six-year study, screws were commonly placed in anterior pillars, paranasal regions, and zygomatic bone, depending on anatomy. Impressions for provisional screw-retained prostheses were taken within 2 to 7 days, while definitive restorations were delivered months later.
That sequence is one reason patients are interested in the method. It can, in selected cases, compress the timeline between surgery and functional teeth. But the ability to deliver provisional teeth early should not be mistaken for proof of long-term success. The engineering may be immediate. The biology still takes time to declare itself.
Subperiosteal implants versus endosteal implants
I see the comparison with conventional implants as the central decision point for patients. Endosteal implants are placed inside bone and are backed by the strongest long-term evidence in implant dentistry. Subperiosteal implants are designed for a narrower set of cases, usually when the bone is too thin, too low, or too compromised for that standard approach. In other words, the comparison is less about which system is universally better and more about which problem each system is built to solve.
| Feature | Subperiosteal implant | Endosteal implant |
|---|---|---|
| Position | On top of jawbone, under periosteum | Inside jawbone |
| Typical use | Severe atrophy, graft-averse or graft-ineligible patients | Patients with adequate bone volume |
| Design | Patient-specific titanium framework | Standardized screw or cylinder implant |
| Surgical goal | Avoid extensive grafting, restore support on deficient ridges | Achieve bone integration within jaw |
| Loading pathway | Sometimes allows early provisionalization | Often requires longer healing depending on case |
| Evidence base | Improving, but still more limited and heterogeneous | Broad, mature, and more predictable long-term |
AAOMS notes that implant reconstructive surgery may be indicated for masticatory dysfunction, speech impairment, esthetic compromise, and alveolar atrophy, goals that matter deeply to patients who have struggled with unstable dentures or severe resorption.
AAOMS states that implant treatment aims to “restore function, improve mastication, speech, deglutition and appearance.”
What the evidence says about success and failure
I would urge any reader to distinguish between short-term survival and long-term durability. The modern literature is promising in the near term, but it is not yet definitive across decades. In the 2024 systematic review of additively manufactured devices, 97.8 percent of implants were functioning at a weighted mean follow-up of 21.4 months. Yet the same review reported partial exposure in 25.6 percent of implants and soft tissue or persistent infection in 5.3 percent of patients.
A broader 2025 systematic review and meta-analysis of full-arch rehabilitation in severely resorbed jaws found encouraging outcomes for one-step, digitally fabricated implants, including 100 percent survival in the pooled one-intervention subgroup over relatively short follow-up periods of 4 to 38 months. By contrast, older two-stage approaches, followed much longer, showed markedly lower survival, including 85 percent overall in that subgroup and much weaker long-range results in historic studies. – subperiosteal implant.
Still, long-term caution is warranted. A 2025 review summarizing older literature reported survival ranges of roughly 90 to 96 percent at five years, 67 to 86 percent at ten years, and substantial attrition thereafter. More soberingly, the 2024 six-year follow-up study of one 3D-printed approach reported major complications in many cases and only a minority of cases classed as fully successful at six years.
One systematic review concluded that modern subperiosteal implants “presented a good survival in the short-time,” while emphasizing the lack of strong medium- and long-term data.
The complications that matter most
I think the most honest way to discuss subperiosteal implants is to say that the danger lies less in the concept than in the interface between metal, soft tissue, and hygiene over time. Historically, the major complications have been framework exposure, recurrent infection, pain, mobility, and progressive bone resorption beneath or around the structure. Older reviews describe a long list of problems, but the recurring theme is breakdown at the soft-tissue barrier and failure of stable adaptation.
Modern systems have improved this, but they have not eliminated it. The 2024 review of additively manufactured implants still found meaningful rates of partial exposure and infection. The 2024 long-term follow-up study linked trouble to exposure of the metal frame, mobility before the first several months, recurrent infections, and inadequate mucoperiosteal integration. It also argued that precise fit, sufficient screw number, and stable positioning in strong bony pillars are critical. – subperiosteal implant.
That is why patient behavior remains part of the treatment. Oral hygiene, smoking status, parafunctional habits, and follow-up compliance are not side notes. They are determinants of whether a customized framework remains merely present or truly serviceable over the years.
Recovery, loading, and daily life after surgery
I would describe recovery as potentially faster than with graft-heavy reconstruction, but not necessarily easy. Because the implant is not being threaded into the jaw like a conventional endosteal fixture, and because it may help patients avoid sinus lifts or large bone grafts, treatment can reduce overall surgical burden in selected cases. Recent reviews and clinical series describe one-step digital protocols in which early or immediate provisionalization is feasible. In the six-year study, impressions for provisional prostheses were often taken within 2 to 7 days after surgery.
That said, early teeth do not mean no healing. Swelling, soreness, soft-tissue adaptation, antibiotic use, and careful hygiene are still part of the immediate postoperative period. The prosthetic sequence may include a provisional restoration first, with definitive CAD/CAM restorations months later. Surgeons must also monitor for pressure points, soft-tissue thinning, or early exposure.
For many patients, what matters most is the return of function. AAOMS describes implant reconstruction broadly as a way to improve mastication, speech, swallowing, and psychological well-being, all of which speak directly to the lived burden of severe tooth loss and unstable dentures.
Cost, access, and the real economics of treatment
I have found that cost discussions around subperiosteal implants are often less transparent than the medical details. There is no universal fee schedule, and pricing varies sharply by country, clinic, prosthetic design, imaging needs, and whether the case is a single arch or a more complex reconstruction. The big economic driver is customization: CBCT imaging, CAD/CAM planning, titanium manufacturing, surgery, and the prosthetic restoration all contribute to the bill.
Published market-facing estimates from 2025 suggest that single-tooth or limited subperiosteal treatment may cost more than standard implants because the framework is custom fabricated, while full-arch prices vary widely in dental tourism settings. Those figures should be treated as examples rather than standards because they come from clinics and treatment brokers, not regulated national fee schedules. – subperiosteal implant.
The more important financial question may be comparative rather than absolute: for a patient otherwise facing staged grafting, sinus augmentation, long healing delays, and multiple surgeries, a subperiosteal plan can sometimes compress treatment even if its upfront price looks high. Whether that tradeoff is worthwhile depends on anatomy, goals, and the surgeon’s experience.
Where the field stands now
I would place subperiosteal implants in the category of selective innovation rather than mainstream replacement. They are not displacing endosteal implants, and the evidence does not justify that. What they are doing is reclaiming a narrow but meaningful role in the rehabilitation of severely resorbed jaws. The 2025 full-arch review called them a “good alternative” for severe atrophy, especially when fabricated digitally in a single step, while also noting the need for more randomized trials and longer follow-up. – subperiosteal implant.
That tension is the honest state of the science. One body of literature shows improved fit, lower morbidity, and strong short-term survival. Another reminds clinicians that biological complications remain common and that some designs may perform poorly over six years. The best current reading is neither triumphalist nor dismissive. It is conditional. In the right patient, with careful design and disciplined follow-up, a subperiosteal implant may restore function where conventional approaches are unrealistic. In the wrong patient, or with weak soft-tissue management, it can fail in exactly the ways that once tarnished its reputation.
Survival and treatment snapshot
| Measure | What recent evidence suggests |
|---|---|
| Historic popularity | Commonly used from the 1940s to the 1980s |
| Modern short-term function | 97.8% of implants in function at mean 21.4 months in one systematic review |
| Common modern complications | Partial exposure and soft-tissue infection remain notable risks |
| One-step digital protocols | Short-term reports include early or immediate loading in selected cases |
| Longer-term uncertainty | Evidence is heterogeneous, and some six-year outcomes are much less favorable |
| Best current indication | Severe jaw atrophy when conventional implants or grafting are unsuitable |
Takeaways
- Subperiosteal implants sit on top of the jawbone under the periosteum rather than inside bone like standard implants.
- They are mainly used for severe jawbone loss when conventional implants or grafting are not suitable.
- Modern versions rely on CBCT imaging, CAD/CAM planning, titanium manufacturing, and fixation screws.
- Short-term survival data are encouraging, but soft-tissue exposure and infection remain major concerns.
- Endosteal implants still have the stronger long-term evidence base for patients with enough bone.
- The best candidates are carefully selected patients with advanced atrophy, good hygiene, and realistic expectations.
- The field is promising but still evolving, with stronger long-term studies still needed.
Conclusion
I come away from the evidence with a view that is optimistic, but only in a disciplined way. Subperiosteal implants are not a miracle workaround for everyone who wants teeth faster. They are a sophisticated salvage strategy for anatomy that no longer cooperates with ordinary implant planning. In that role, they matter. – subperiosteal implant.
Their modern revival makes sense. Digital design has improved fit. Titanium frameworks and fixation strategies have improved stability. One-step workflows can reduce the burden of care for people who would otherwise face long, invasive reconstruction. For some patients, that is not a cosmetic convenience but a serious restoration of chewing, speech, appearance, and confidence.
But the older warnings have not vanished. Soft-tissue breakdown, exposure, infection, and mobility still define the limits of success. The literature is strongest in the short term and still unsettled in the long term. That means the future of subperiosteal implants will depend less on hype than on case selection, surgical judgment, prosthetic discipline, and honest follow-up. For the right patient, the option is real. For the field as a whole, the verdict is still being written. – subperiosteal implant.
FAQs
What is the main difference between a subperiosteal implant and a regular implant?
A subperiosteal implant sits on top of the jawbone under the periosteum, while a regular endosteal implant is placed inside the bone. Subperiosteal systems are usually reserved for patients with severe bone loss.
Are subperiosteal implants safe?
They can be safe and effective in carefully selected cases, especially with modern digital design, but they carry meaningful risks such as exposure, infection, and mobility. Safety depends heavily on anatomy, hygiene, and surgical experience.
Do subperiosteal implants require bone grafting?
Usually, they are considered specifically when clinicians want to avoid major grafting or when grafting is not feasible. That is one of their main advantages in severe jaw atrophy.
How long do subperiosteal implants last?
Short-term outcomes can be strong, but long-term durability is more variable than for conventional implants. Modern data are encouraging in the first few years, while older and some longer follow-up studies show more complications over time.
Can teeth be attached quickly after surgery?
Sometimes, yes. In selected digital workflows, provisional teeth may be started within days, but this depends on the design, stability, and surgeon’s protocol. Early loading is possible, not guaranteed.